|
|
|
Lung transplantation for bronchiolitis obliterans syndrome after allogenic hematopoietic stem cell transplantation |
Fei Gao1, Jingyu Chen2( ), Dong Wei2, Bo Wu2, Min Zhou2 ), Dong Wei2, Bo Wu2, Min Zhou2 |
1. Department of Emergency, Jiangsu Key Lab of Organ Transplantation, Nanjing Medical University, Affiliated Wuxi People’s Hospital, Wuxi 214000, China
2. Transplantation Center, Jiangsu Key Lab of Organ Transplantation, Nanjing Medical University, Affiliated Wuxi People’s Hospital, Wuxi 214000, China |
|
|
|
|
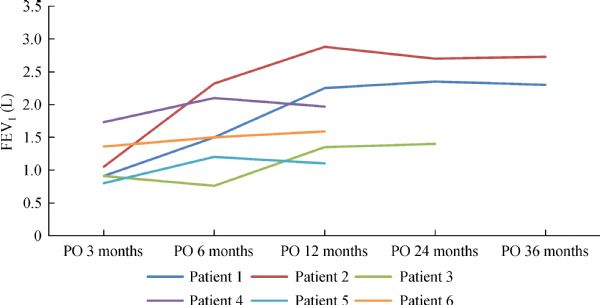
Abstract Bronchiolitis obliterans syndrome (BOS) after hematopoietic stem cell transplantation (HSCT) is a major cause of morbidity and mortality with limited treatment options. Lung transplantation (LTX) has been rarely reported as a treatment option for selected HSCT recipients with this problem. In the present study, we reported six patients who underwent LTX due to BOS after HSCT (two females, four males) from January 2012 to December 2014 in our center. The median time from HSCT to diagnosis of BOS was 2.5 years (ranging from 1 to 5 years). At a median time of 4 years (ranging from 2 to 5 years) after diagnosis of BOS, four patients received bilateral sequential LTX, and two patients received single LTX. One of the recipients suffered from mild acute rejection after LTX, another suffered from primary lung graft dysfunction on post-operation day 2, and three experienced fungal infections. The median time for follow-up after LTX was 19.5 months (ranging from 12 to 39 months). At present, all patients are alive with good functional capacity and no relapse of BOS and hematologic malignancy conditions. Patients who received bilateral LTX have better pulmonary functions than patients who received single LTX.
|
| Keywords
bronchiolitis obliterans syndrome (BOS)
hematopoietic stem cell transplantation (HSCT)
lung transplantation (LTX)
|
|
Corresponding Author(s):
Jingyu Chen
|
|
Just Accepted Date: 07 July 2017
Online First Date: 28 July 2017
Issue Date: 02 April 2018
|
|
| 1 |
Palmas A, Tefferi A, Myers JL, Scott JP, Swensen SJ, Chen MG, Gastineau DA, Gertz MA, Inwards DJ, Lacy MQ, Litzow MR. Late-onset noninfectious pulmonary complications after allogeneic bone marrow transplantation. Br J Haematol 1998; 100(4): 680–687
https://doi.org/10.1046/j.1365-2141.1998.00617.x
pmid: 9531334
|
| 2 |
Afessa B, Peters SG. Chronic lung disease after hematopoietic stem cell transplantation. Clin Chest Med 2005; 26(4): 571–586
https://doi.org/10.1016/j.ccm.2005.06.012
pmid: 16263397
|
| 3 |
Au BK, Au MA, Chien JW. Bronchiolitis obliterans syndrome epidemiology after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant 2011; 17(7): 1072–1078
https://doi.org/10.1016/j.bbmt.2010.11.018
pmid: 21126596
|
| 4 |
Soubani AO, Uberti JP. Bronchiolitis obliterans following haematopoietic stem cell transplantation. Eur Respir J 2007; 29(5): 1007–1019
https://doi.org/10.1183/09031936.00052806
pmid: 17470622
|
| 5 |
Redel-Montero J, Bujalance-Cabrera C, Vaquero-Barrios JM, Santos-Luna F, Arenas-De Larriva M, Moreno-Casado P, Espinosa-Jiménez D. Lung transplantation for bronchiolitis obliterans after allogenic bone marrow transplantation. Transplant Proc 2010; 42(8): 3023–3025
https://doi.org/10.1016/j.transproceed.2010.07.086
pmid: 20970599
|
| 6 |
Sakaida E, Nakaseko C, Harima A, Yokota A, Cho R, Saito Y, Nishimura M. Late-onset noninfectious pulmonary complications after allogeneic stem cell transplantation are significantly associated with chronic graft-versus-host disease and with the graft-versus-leukemia effect. Blood 2003; 102(12): 4236–4242
https://doi.org/10.1182/blood-2002-10-3289
pmid: 12907447
|
| 7 |
Dudek AZ, Mahaseth H, DeFor TE, Weisdorf DJ. Bronchiolitis obliterans in chronic graft-versus-host disease: analysis of risk factors and treatment outcomes. Biol Blood Marrow Transplant 2003; 9(10): 657–666
https://doi.org/10.1016/S1083-8791(03)00242-8
pmid: 14569562
|
| 8 |
Holm AM, Riise GC, Hansson L, Brinch L, Bjørtuft O, Iversen M, Simonsen S, Fløisand Y. Lung transplantation for bronchiolitis obliterans syndrome after allo-SCT. Bone Marrow Transplant 2013; 48(5): 703–707
https://doi.org/10.1038/bmt.2012.197
pmid: 23064037
|
| 9 |
Vogl UM, Nagayama K, Bojic M, Hoda MA, Klepetko W, Jaksch P, Dekan S, Siersch V, Mitterbauer M, Schellongowski P, Greinix HT, Petkov V, Schulenburg A, Kalhs P, Rabitsch W. Lung transplantation for bronchiolitis obliterans after allogeneic hematopoietic stem cell transplantation: a single-center experience. Transplantation 2013; 95(4): 623–628
https://doi.org/10.1097/TP.0b013e318277e29e
pmid: 23274967
|
| 10 |
Rampolla R. Lung transplantation: an overview of candidacy and outcomes. Ochsner J 2014; 14(4): 641–648
pmid: 25598729
|
| 11 |
Soubani AO, Kingah P, Alshabani K, Muma G, Haq A. Lung transplantation following hematopoietic stem cell transplantation: report of two cases and systematic review of literature. Clin Transplant 2014; 28(7): 776–782
https://doi.org/10.1111/ctr.12378
pmid: 24754643
|
| 12 |
van den Brink MR, Porter DL, Giralt S, Lu SX, Jenq RR, Hanash A, Bishop MR. Relapse after allogeneic hematopoietic cell therapy. Biol Blood Marrow Transplant 2010; 16(1 Suppl): S138–S145
https://doi.org/10.1016/j.bbmt.2009.10.023
pmid: 19857588
|
| 13 |
Palmer SM, Miralles AP, Lawrence CM, Gaynor JW, Davis RD, Tapson VF. Rabbit antithymocyte globulin decreases acute rejection after lung transplantation: results of a randomized, prospective study. Chest 1999; 116(1): 127–133
https://doi.org/10.1378/chest.116.1.127
pmid: 10424515
|
| 14 |
Garrity ER Jr, Villanueva J, Bhorade SM, Husain AN, Vigneswaran WT. Low rate of acute lung allograft rejection after the use of daclizumab, an interleukin 2 receptor antibody. Transplantation 2001; 71(6): 773–777
https://doi.org/10.1097/00007890-200103270-00015
pmid: 11330541
|
| 15 |
Hartwig MG, Snyder LD, Appel JZ 3rd, Cantu E 3rd, Lin SS, Palmer SM, Davis RD. Rabbit anti-thymocyte globulin induction therapy does not prolong survival after lung transplantation. J Heart Lung Transplant 2008; 27(5): 547–553
https://doi.org/10.1016/j.healun.2008.01.022
pmid: 18442722
|
| 16 |
Hartert M, Senbaklavacin O, Gohrbandt B, Fischer BM, Buhl R, Vahld CF. Lung transplantation: a treatment option in end-stage lung disease. Dtsch Arztebl Int 2014; 111(7): 107–116
pmid: 24622680
|
| 17 |
Gabardi S, Kubiak DW, Chandraker AK, Tullius SG. Invasive fungal infections and antifungal therapies in solid organ transplant recipients. Transpl Int 2007; 20(12): 993–1015
https://doi.org/10.1111/j.1432-2277.2007.00511.x
pmid: 17617181
|
| 18 |
Solé A, Morant P, Salavert M, Pemán J, Morales P; Valencia Lung Transplant Group. Aspergillus infections in lung transplant recipients: risk factors and outcome. Clin Microbiol Infect 2005; 11(5): 359–365
https://doi.org/10.1111/j.1469-0691.2005.01128.x
pmid: 15819861
|
| 19 |
Solé A, Salavert M. Fungal infections after lung transplantation. Transplant Rev (Orlando) 2008; 22(2): 89–104
https://doi.org/10.1016/j.trre.2007.12.007
pmid: 18631862
|
|
Viewed |
|
|
|
Full text
|
|
|
|
|
Abstract
|
|
|
|
|
Cited |
|
|
|
|
| |
Shared |
|
|
|
|
| |
Discussed |
|
|
|
|