| LETTER TO FRONTIERS OF MEDICINE |
|
|
|
Learning curve of totally thoracoscopic pulmonary segmentectomy |
Weibing Wu, Jing Xu, Wei Wen, Yue Yu, Xinfeng Xu, Quan Zhu( ), Liang Chen() ), Liang Chen() |
| Department of Thoracic Surgery, The First Affiliated Hospital of Nanjing Medical University, Nanjing 210029, China |
|
|
|
|
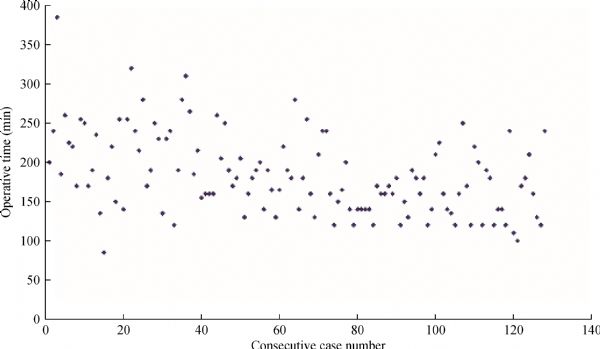
Abstract Totally thoracoscopic pulmonary segmentectomy (TTPS) is a feasible and safe technique that requires advanced thoracoscopic skills and knowledge of pulmonary anatomy. However, data describing the learning curve of TTPS have yet to be obtained. In this study, 128 patients who underwent TTPS between September 2010 and December 2013 were retrospectively analyzed to evaluate the learning curve and were divided chronologically into three phases, namely, ascending phase (A), plateau phase (B), and descending phase (C), through cumulative summation (CUSUM) for operative time (OT). Phases A, B, and C comprised 39, 33, and 56 cases, respectively. OT and blood loss decreased significantly from phases A to C (P <0.01), and the frequency of intraoperative bronchoscopy for target bronchus identification decreased gradually (A, 8/39; B, 4/33; C, 3/56; P = 0.06). No significant differences were observed in demographic factors, conversion, complications, hospital stay, and retrieved lymph nodes among the three phases. Surgical outcomes and techniques improved with experience and volume. CUSUMOT indicated that the learning curve of TTPS should be more than 72 cases.
|
| Keywords
thoracoscopic
segmentectomy
learning curve
CUSUM
|
|
Corresponding Author(s):
Quan Zhu,Liang Chen
|
|
Just Accepted Date: 12 December 2017
Online First Date: 26 February 2018
Issue Date: 29 September 2018
|
|
| 1 |
Churchill ED, Belsey R. Segmental pneumonectomy in bronchiectasis: the lingual segment of the left upper lobe. Ann Surg 1939; 109(4): 481–499
https://doi.org/10.1097/00000658-193904000-00001
pmid: 17857340
|
| 2 |
Schuchert MJ, Abbas G, Awais O, Pennathur A, Nason KS, Wilson DO, Siegfried JM, Luketich JD, Landreneau RJ. Anatomic segmentectomy for the solitary pulmonary nodule and early-stage lung cancer. Ann Thorac Surg 2012; 93(6): 1780–1787, discussion 1786–1787
https://doi.org/10.1016/j.athoracsur.2011.11.074
pmid: 22483652
|
| 3 |
Landreneau RJ, Normolle DP, Christie NA, Awais O, Wizorek JJ, Abbas G, Pennathur A, Shende M, Weksler B, Luketich JD, Schuchert MJ. Recurrence and survival outcomes after anatomic segmentectomy versus lobectomy for clinical stage I non-small-cell lung cancer: a propensity-matched analysis. J Clin Oncol 2014; 32(23): 2449–2455
https://doi.org/10.1200/JCO.2013.50.8762
pmid: 24982447
|
| 4 |
Okada M, Nishio W, Sakamoto T, Uchino K, Yuki T, Nakagawa A, Tsubota N. Effect of tumor size on prognosis in patients with non-small cell lung cancer: the role of segmentectomy as a type of lesser resection. J Thorac Cardiovasc Surg 2005; 129(1): 87–93
https://doi.org/10.1016/j.jtcvs.2004.04.030
pmid: 15632829
|
| 5 |
Yamashita S, Tokuishi K, Anami K, Moroga T, Miyawaki M, Chujo M, Yamamoto S, Kawahara K. Thoracoscopic segmentectomy for T1 classification of non-small cell lung cancer: a single center experience. Eur J Cardiothorac Surg 2012; 42(1): 83–88
https://doi.org/10.1093/ejcts/ezr254
pmid: 22228839
|
| 6 |
Harada H, Okada M, Sakamoto T, Matsuoka H, Tsubota N. Functional advantage after radical segmentectomy versus lobectomy for lung cancer. Ann Thorac Surg 2005; 80(6): 2041–2045
https://doi.org/10.1016/j.athoracsur.2005.06.010
pmid: 16305841
|
| 7 |
Yoshimoto K, Nomori H, Mori T, Ohba Y, Shibata H, Tashiro K, Shiraishi S, Kobayashi T. A segmentectomy of the right upper lobe has an advantage over a right upper lobectomy regarding the preservation of the functional volume of the right middle lobe: analysis by perfusion single-photon emission computed tomography/computed tomography. Surg Today 2010; 40(7): 614–619
https://doi.org/10.1007/s00595-009-4103-9
pmid: 20582511
|
| 8 |
Wisnivesky JP, Henschke CI, Swanson S, Yankelevitz DF, Zulueta J, Marcus S, Halm EA. Limited resection for the treatment of patients with stage IA lung cancer. Ann Surg 2010; 251(3): 550–554
https://doi.org/10.1097/SLA.0b013e3181c0e5f3
pmid: 20160639
|
| 9 |
Atkins BZ, Harpole DH Jr, Mangum JH, Toloza EM, D’Amico TA, Burfeind WR Jr. Pulmonary segmentectomy by thoracotomy or thoracoscopy: reduced hospital length of stay with a minimally-invasive approach. Ann Thorac Surg 2007; 84(4): 1107–1113
https://doi.org/10.1016/j.athoracsur.2007.05.013
pmid: 17888955
|
| 10 |
Schuchert MJ, Pettiford BL, Pennathur A, Abbas G, Awais O, Close J, Kilic A, Jack R, Landreneau JR, Landreneau JP, Wilson DO, Luketich JD, Landreneau RJ. Anatomic segmentectomy for stage I non-small-cell lung cancer: comparison of video-assisted thoracic surgery versus open approach. J Thorac Cardiovasc Surg 2009; 138(6): 1318–25.e1
https://doi.org/10.1016/j.jtcvs.2009.08.028
pmid: 19931665
|
| 11 |
Watanabe A, Ohori S, Nakashima S, Mawatari T, Inoue N, Kurimoto Y, Higami T. Feasibility of video-assisted thoracoscopic surgery segmentectomy for selected peripheral lung carcinomas. Eur J Cardiothorac Surg 2009; 35(5): 775–780, discussion 780
https://doi.org/10.1016/j.ejcts.2009.01.013
pmid: 19231231
|
| 12 |
Oizumi H, Kanauchi N, Kato H, Endoh M, Takeda S, Suzuki J, Fukaya K, Sadahiro M. Total thoracoscopic pulmonary segmentectomy. Eur J Cardiothorac Surg 2009; 36(2): 374–377, discussion 377
https://doi.org/10.1016/j.ejcts.2009.03.038
pmid: 19442531
|
| 13 |
Leshnower BG, Miller DL, Fernandez FG, Pickens A, Force SD. Video-assisted thoracoscopic surgery segmentectomy: a safe and effective procedure. Ann Thorac Surg 2010; 89(5): 1571–1576
https://doi.org/10.1016/j.athoracsur.2010.01.061
pmid: 20417779
|
| 14 |
Gossot D, Ramos R, Brian E, Raynaud C, Girard P, Strauss C. A totally thoracoscopic approach for pulmonary anatomic segmentectomies. Interact Cardiovasc Thorac Surg 2011; 12(4): 529–533
https://doi.org/10.1510/icvts.2010.257493
pmid: 21239448
|
| 15 |
Yang CF, D’Amico TA. Thoracoscopic segmentectomy for lung cancer. Ann Thorac Surg 2012; 94(2): 668–681
https://doi.org/10.1016/j.athoracsur.2012.03.080
pmid: 22748648
|
| 16 |
Oizumi H, Kanauchi N, Kato H, Endoh M, Suzuki J, Fukaya K, Sadahiro M. Anatomic thoracoscopic pulmonary segmentectomy under 3-dimensional multidetector computed tomography simulation: a report of 52 consecutive cases. J Thorac Cardiovasc Surg 2011; 141(3): 678–682
https://doi.org/10.1016/j.jtcvs.2010.08.027
pmid: 20884021
|
| 17 |
Bokhari MB, Patel CB, Ramos-Valadez DI, Ragupathi M, Haas EM. Learning curve for robotic-assisted laparoscopic colorectal surgery. Surg Endosc 2011; 25(3): 855–860
https://doi.org/10.1007/s00464-010-1281-x
pmid: 20734081
|
| 18 |
Liao HJ, Dong C, Kong FJ, Zhang ZP, Huang P, Chang S. The CUSUM analysis of the learning curve for endoscopic thyroidectomy by the breast approach. Surg Innov 2014; 21(2): 221–228
https://doi.org/10.1177/1553350613500722
pmid: 23965590
|
| 19 |
McKenna RJ Jr. Complications and learning curves for video-assisted thoracic surgery lobectomy. Thorac Surg Clin 2008; 18(3): 275–280
https://doi.org/10.1016/j.thorsurg.2008.04.004
pmid: 18831503
|
| 20 |
Zhao H, Bu L, Yang F, Li J, Li Y, Wang J. Video-assisted thoracoscopic surgery lobectomy for lung cancer: the learning curve. World J Surg 2010; 34(10): 2368–2372
https://doi.org/10.1007/s00268-010-0661-7
pmid: 20567972
|
| 21 |
Meyer M, Gharagozloo F, Tempesta B, Margolis M, Strother E, Christenson D. The learning curve of robotic lobectomy. Int J Med Robot 2012; 8(4): 448–452
https://doi.org/10.1002/rcs.1455
pmid: 22991294
|
| 22 |
Guo W, Zou YB, Ma Z, Niu HJ, Jiang YG, Zhao YP, Gong TQ, Wang RW. One surgeon’s learning curve for video-assisted thoracoscopic esophagectomy for esophageal cancer with the patient in lateral position: how many cases are needed to reach competence? Surg Endosc 2013; 27(4): 1346–1352
https://doi.org/10.1007/s00464-012-2614-8
pmid: 23093242
|
| 23 |
Williams SM, Parry BR, Schlup MM. Quality control: an application of the cusum. BMJ 1992; 304(6838): 1359–1361
https://doi.org/10.1136/bmj.304.6838.1359
pmid: 1611337
|
| 24 |
Mawatari T, Murakami G, Koshino T, Morishita K, Abe T. Posterior pulmonary lobe: segmental and vascular anatomy in human specimens. Clin Anat 2000; 13(4): 257–262
https://doi.org/10.1002/1098-2353(2000)13:4<257::AID-CA5>3.0.CO;2-5
pmid: 10873217
|
|
Viewed |
|
|
|
Full text
|
|
|
|
|
Abstract
|
|
|
|
|
Cited |
|
|
|
|
| |
Shared |
|
|
|
|
| |
Discussed |
|
|
|
|