|
|
|
SinoSCORE: a logistically derived additive prediction model for post-coronary artery bypass grafting in-hospital mortality in a Chinese population |
Zhe Zheng( ), Lu Zhang, Xi Li, Shengshou Hu(), on behalf of the Chinese CABG Registry Study ), Lu Zhang, Xi Li, Shengshou Hu(), on behalf of the Chinese CABG Registry Study |
| Department of Cardiovascular Surgery and State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100037, China |
|
|
|
|
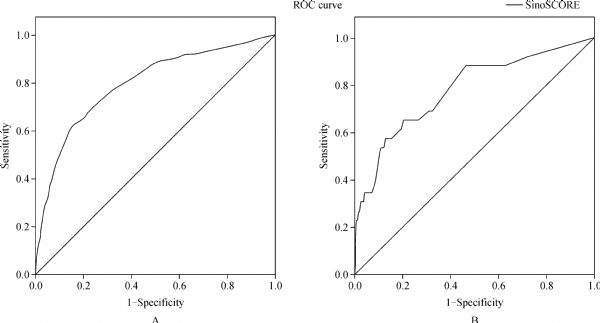
Abstract This study aims to construct a logistically derived additive score for predicting in-hospital mortality risk in Chinese patients undergoing coronary artery bypass surgery (CABG). Data from 9839 consecutive CABG patients in 43 Chinese centers were collected between 2007 and 2008 from the Chinese Coronary Artery Bypass Grafting Registry. This database was randomly divided into developmental and validation subsets (9:1). The data in the developmental dataset were used to develop the model using logistic regression. Calibration and discrimination characteristics were assessed using the validation dataset. Thresholds were defined for each model to distinguish different risk groups. After excluding 275 patients with incomplete information, the overall mortality rate of the remaining 9564 patients was 2.5%. The SinoSCORE model was constructed based on 11 variables: age, preoperative NYHA stage III or IV, chronic renal failure, extracardiac arteriopathy, chronic obstructive pulmonary disease, preoperative atrial fibrillation or flutter (within 2βweeks), left ventricular ejection fraction, other elective surgery, combined valve procedures, preoperative critical state, and BMI. In the developmental dataset, calibration using a Hosmer-Lemeshow (HL) test was at P =β0.44 and discrimination based on the area under the receiver operating characteristic curve (ROC) was 0.80. In the validation dataset, the HL test was at P =β0.34 and the area under the ROC (AUC) was 0.78. A logistically derived additive model for predicting in-hospital mortality among Chinese patients undergoing CABG was developed based on the most up-to-date multi-center data from China.
|
| Keywords
coronary artery bypass grafting
risk stratification
in-hospital mortality
|
|
Corresponding Author(s):
Zheng Zhe,Email:zhengzhe@fuwai.com; Hu Shengshou,Email:shengshouhu@yahoo.com
|
|
Issue Date: 05 December 2013
|
|
| 1 |
Hannan EL, Siu AL, Kumar D, Racz M, Pryor DB, Chassin MR. Assessment of coronary artery bypass graft surgery performance in New York. Is there a bias against taking high-risk patients? Med Care 1997; 35(1): 49–56
doi: 10.1097/00005650-199701000-00004 pmid:8998202
|
| 2 |
Edwards FH, Grover FL, Shroyer AL, Schwartz M, Bero J. The Society of Thoracic Surgeons National Cardiac Surgery Database: current risk assessment. Ann Thorac Surg 1997; 63(3): 903–908
doi: 10.1016/S0003-4975(97)00017-9 pmid:9066436
|
| 3 |
Parsonnet V, Dean D, Bernstein AD. A method of uniform stratification of risk for evaluating the results of surgery in acquired adult heart disease. Circulation 1989; 79(6 Pt 2 suppl I): I3–I12
pmid:2720942
|
| 4 |
Eagle KA, Guyton RA, Davidoff R, Ewy GA, Fonger J, Gardner TJ, Gott JP, Herrmann HC, Marlow RA, Nugent W, O’Connor GT, Orszulak TA, Rieselbach RE, Winters WL, Yusuf S, Gibbons RJ, Alpert JS, Garson A Jr, Gregoratos G, Russell RO, Ryan TJ, Smith SC Jr. ACC/AHA guidelines for coronary artery bypass graft surgery: executive summary and recommendations : A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to revise the 1991 guidelines for coronary artery bypass graft surgery). Circulation 1999; 100(13): 1464–1480
doi: 10.1161/01.CIR.100.13.1464 pmid:10500052
|
| 5 |
Roques F, Nashef SAM, Michel P, Gauducheau E, de Vincentiis C, Baudet E, Cortina J, David M, Faichney A, Gabrielle F, Gams E, Harjula A, Jones MT, Pintor PP, Salamon R, Thulin L. Risk factors and outcome in European cardiac surgery: analysis of the EuroSCORE multinational database of 19030 patients. Eur J Cardiothorac Surg 1999; 15(6): 816–822, discussion 822–823
doi: 10.1016/S1010-7940(99)00106-2 pmid:10431864
|
| 6 |
Nashef SA, Roques F, Michel P, Gauducheau E, Lemeshow S, Salamon R. European system for cardiac operative risk evaluation (EuroSCORE). Eur J Cardiothorac Surg 1999; 16(1): 9–13
doi: 10.1016/S1010-7940(99)00134-7 pmid:10456395
|
| 7 |
Mikkelsen MM, Johnsen SP, Nielsen PH, Jakobsen CJ. The EuroSCORE in western Denmark: a population-based study. J Cardiothorac Vasc Anesth 2012; 26(2): 258–264
doi: 10.1053/j.jvca.2011.09.012 pmid:22100858
|
| 8 |
Akar AR, Kurtcephe M, Sener E, Alhan C, Durdu S, Kunt AG, Güvenir HA; Group for the Turkish Society of Cardiovascular Surgery and Turkish Ministry of Health. Validation of the EuroSCORE risk models in Turkish adult cardiac surgical population. Eur J Cardiothorac Surg 2011; 40(3): 730–735
pmid:21342767
|
| 9 |
Parolari A, Pesce LL, Trezzi M, Loardi C, Kassem S, Brambillasca C, Miguel B, Tremoli E, Biglioli P, Alamanni F. Performance of EuroSCORE in CABG and off-pump coronary artery bypass grafting: single institution experience and meta-analysis. Eur Heart J 2009; 30(3): 297–304
doi: 10.1093/eurheartj/ehn581 pmid:19141560
|
| 10 |
Okrainec K, Banerjee DK, Eisenberg MJ. Coronary artery disease in the developing world. Am Heart J 2004; 148(1): 7–15
doi: 10.1016/j.ahj.2003.11.027 pmid:15215786
|
| 11 |
Hu SS. Coronary heart diseases. In: Hu SS, Kong LZ, editors. Annual report 2005 on cardiovascular diseases in China (English edition) . Beijing: Encyclopedia of China Publishing House. 2007: 45–62
|
| 12 |
Zheng Z, Li Y, Zhang S, Hu S; Chinese CABG Registry Study. The Chinese coronary artery bypass grafting registry study: how well does the EuroSCORE predict operative risk for Chinese population? Eur J Cardiothorac Surg 2009; 35(1): 54–58
doi: 10.1016/j.ejcts.2008.08.001 pmid:18778949
|
| 13 |
Li Y, Zheng Z, Hu S; Chinese Coronary Artery Bypass Grafting Registry Study. The Chinese coronary artery bypass grafting registry study: analysis of the national multicentre database of 9248 patients. Heart 2009; 95(14): 1140–1144
doi: 10.1136/hrt.2008.146563 pmid:18632834
|
| 14 |
Moran A, Gu D, Zhao D, Coxson P, Wang YC, Chen CS, Liu J, Cheng J, Bibbins-Domingo K, Shen YM, He J, Goldman L. Future cardiovascular disease in china: Markov model and risk factor scenario projections from the coronary heart disease policy model-china. Circ Cardiovasc Qual Outcomes 2010; 3(3): 243–252
doi: 10.1161/CIRCOUTCOMES.109.910711 pmid:20442213
|
| 16 |
Gopaldas RR, Chu D, Cornwell LD, Dao TK, LeMaire SA, Coselli JS, Bakaeen FG. Cirrhosis as a Moderator of Outcomes in CABG and OPCAB Operations: A 12-Year Population-Based Study. STS/AATS Tech-Con 2013 and STS 49th Annual Meeting. abstract
|
| 17 |
Shroyer AL, Grover FL, Hattler B, Collins JF, McDonald GO, Kozora E, Lucke JC, Baltz JH, Novitzky D; Veterans Affairs Randomized On/Off Bypass (ROOBY) Study Group. On-pump versus off-pump coronary-artery bypass surgery. N Engl J Med 2009; 361(19): 1827–1837
doi: 10.1056/NEJMoa0902905 pmid:19890125
|
| 18 |
Lamy A, Devereaux PJ, Prabhakaran D, Hu S, Piegas LS, Straka Z, Paolasso E, Taggart D, Lanas F, Akar AR, Jain A, Noiseux N, Ou Y, Chrolavicius S, Ng J, Yusuf S. Rationale and design of the coronary artery bypass grafting surgery off or on pump revascularization study: a large international randomized trial in cardiac surgery. Am Heart J 2012; 163(1): 1–6
doi: 10.1016/j.ahj.2011.10.007 pmid:22172429
|
| 19 |
Hannan EL, Wu C, Bennett EV, Carlson RE, Culliford AT, Gold JP, Higgins RS, Isom OW, Smith CR, Jones RH. Risk stratification of in-hospital mortality for coronary artery bypass graft surgery. J Am Coll Cardiol 2006; 47(3): 661–668
doi: 10.1016/j.jacc.2005.10.057 pmid:16458152
|
| 20 |
Carosella VC, Navia JL, Al-Ruzzeh S, Grancelli H, Rodriguez W, Cardenas C, Bilbao J, Nojek C. The first Latin-American risk stratification system for cardiac surgery: can be used as a graphic pocket-card score. Interact Cardiovasc Thorac Surg 2009; 9(2): 203–208
doi: 10.1510/icvts.2008.199083 pmid:19454412
|
| 21 |
Peterson ED, Coombs LP, Ferguson TB, Shroyer AL, DeLong ER, Grover FL, Edwards FH. Hospital variability in length of stay after coronary artery bypass surgery: results from the Society of Thoracic Surgeon’s National Cardiac Database. Ann Thorac Surg 2002; 74(2): 464–473
doi: 10.1016/S0003-4975(02)03694-9 pmid:12173830
|
|
Viewed |
|
|
|
Full text
|
|
|
|
|
Abstract
|
|
|
|
|
Cited |
|
|
|
|
| |
Shared |
|
|
|
|
| |
Discussed |
|
|
|
|