|
|
|
New definition of metabolic dysfunction-associated fatty liver disease with elevated brachial-ankle pulse wave velocity and albuminuria: a prospective cohort study |
Jialu Wang1,2, Shanshan Liu1,2, Qiuyu Cao1,2, Shujing Wu1,2, Jingya Niu1,2, Ruizhi Zheng1,2, Lizhan Bie1,2, Zhuojun Xin1,2, Yuanyue Zhu1,2, Shuangyuan Wang1,2, Hong Lin1,2, Tiange Wang1,2, Min Xu1,2, Jieli Lu1,2, Yuhong Chen1,2, Yiping Xu3, Weiqing Wang1,2, Guang Ning1,2, Yu Xu1,2, Mian Li1,2( ), Yufang Bi1,2(), Zhiyun Zhao1,2() ), Yufang Bi1,2(), Zhiyun Zhao1,2() |
1. Department of Endocrine and Metabolic Diseases, Shanghai Institute of Endocrine and Metabolic Diseases, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200025, China
2. Shanghai National Clinical Research Center for Metabolic Diseases, Key Laboratory for Endocrine and Metabolic Diseases of the National Health Commission of the PR China, Shanghai Key Laboratory for Endocrine Tumor, State Key Laboratory of Medical Genomics, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200025, China
3. Clinical Trials Center, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200025, China |
|
|
|
|
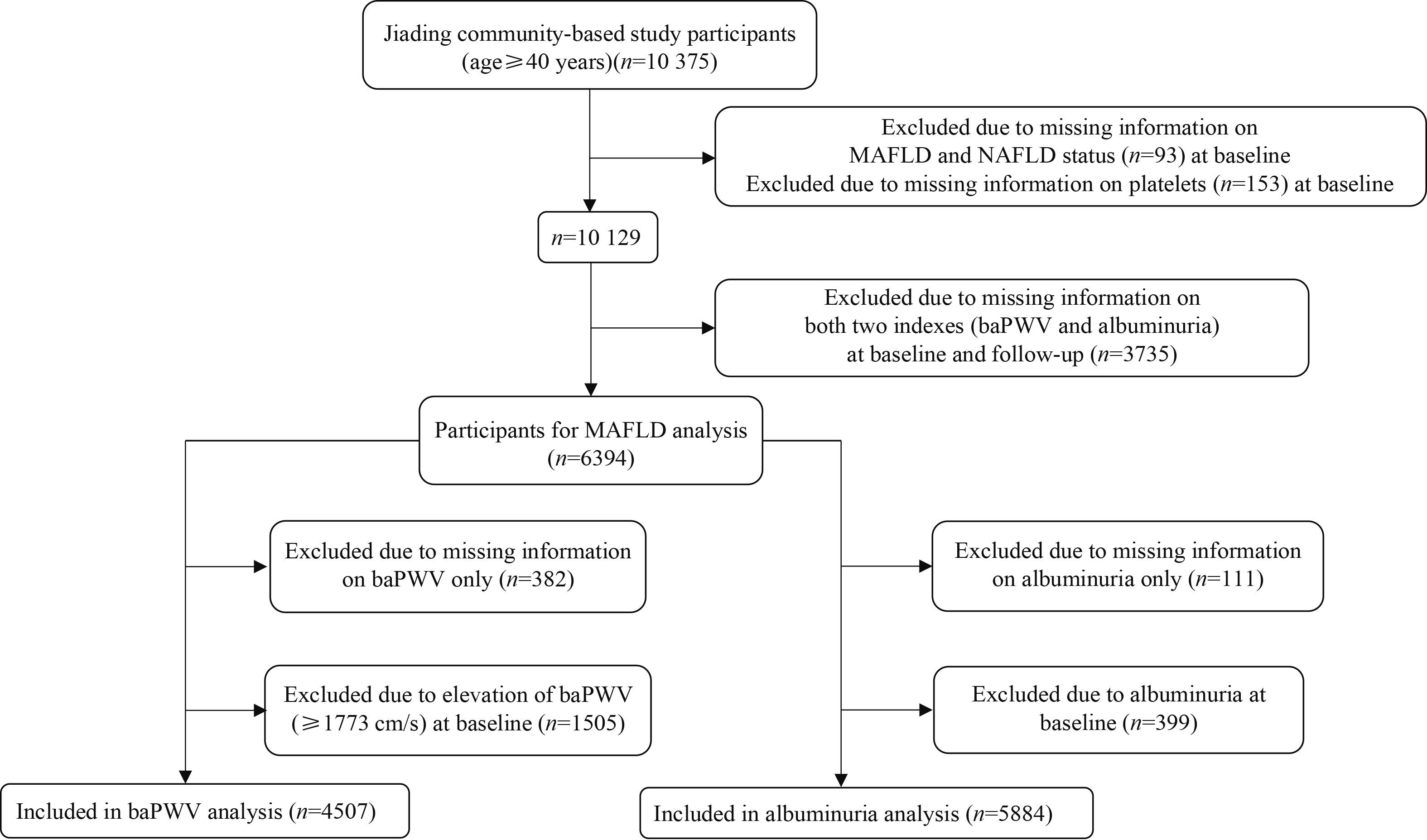
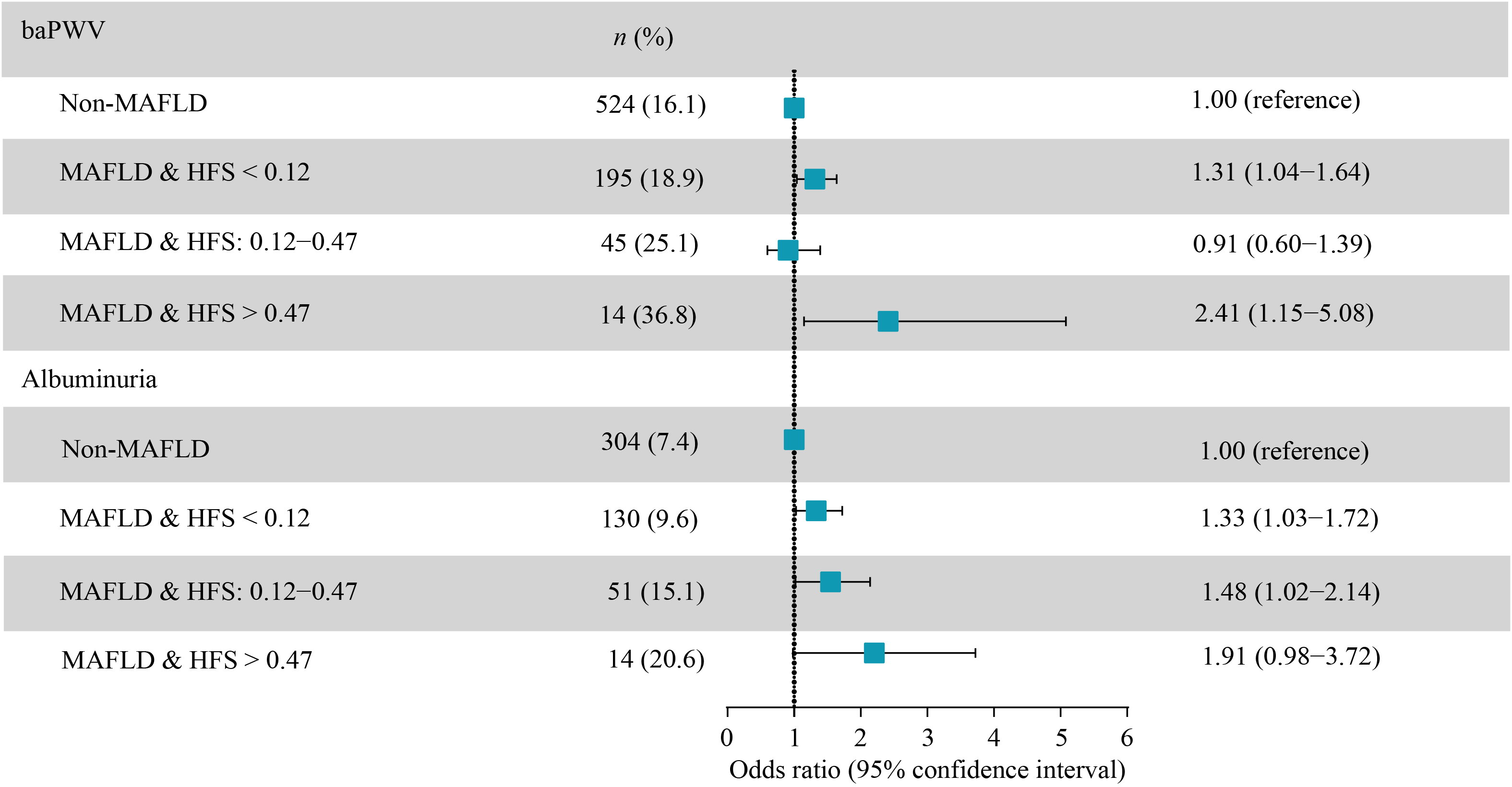
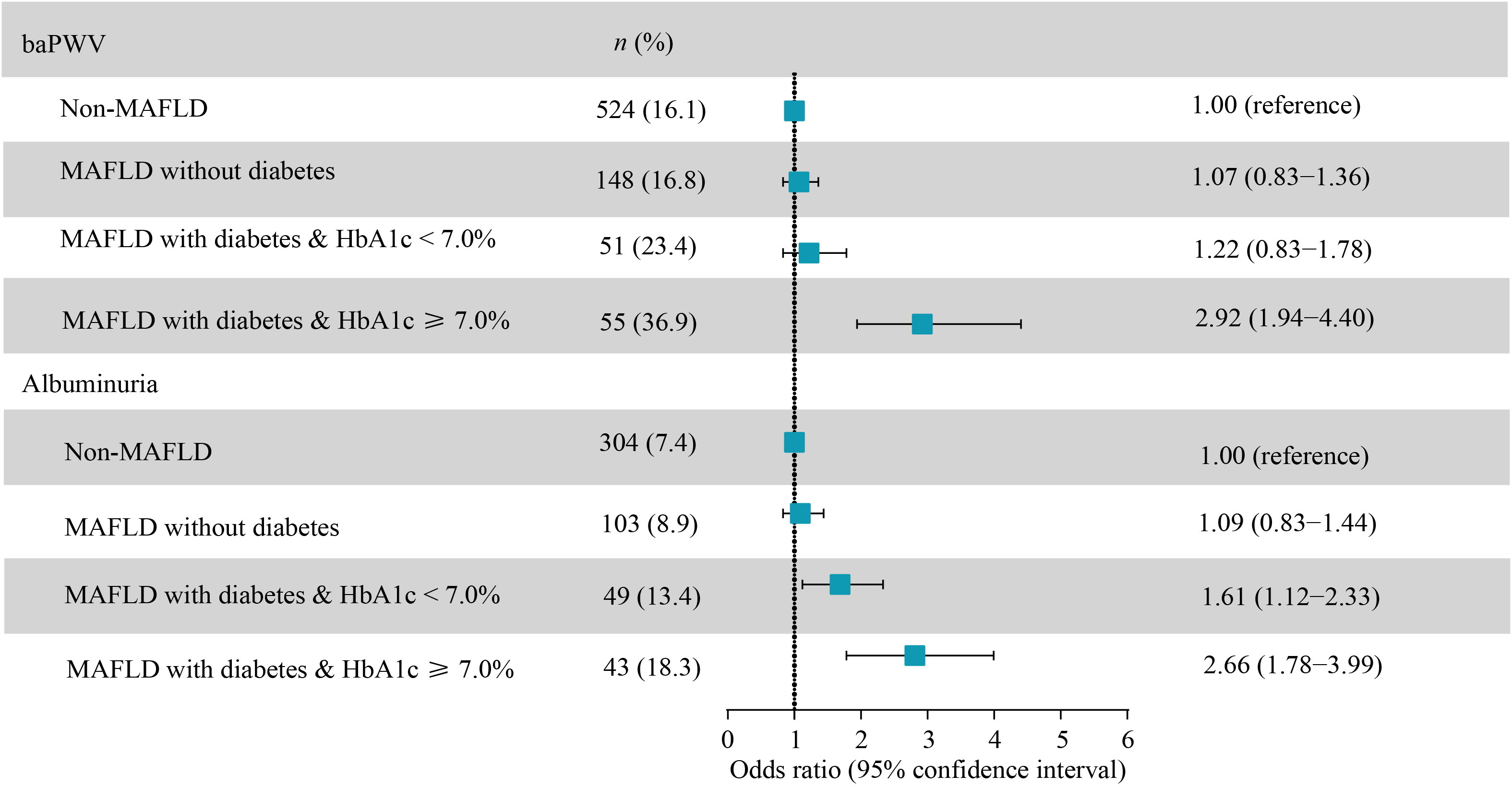
Abstract A new definition of metabolic dysfunction-associated fatty liver disease (MAFLD) has recently been proposed. We aim to examine the associations of MAFLD, particularly its discordance from non-alcoholic fatty liver disease (NAFLD), with the progression of elevated brachial-ankle pulse wave velocity (baPWV) and albuminuria in a community-based study sample in Shanghai, China. After 4.3 years of follow-up, 778 participants developed elevated baPWV and 499 developed albuminuria. In comparison with the non-MAFLD group, the multivariable adjusted odds ratio (OR) of MAFLD group for new-onset elevated baPWV was 1.25 (95% confidence interval (CI) 1.01–1.55) and 1.35 (95% CI 1.07–1.70) for albuminuria. Participants without NAFLD but diagnosed according to MAFLD definition were associated with higher risk of incident albuminuria (OR 1.77; 95% CI 1.07–2.94). Patients with MAFLD with high value of hepamet fibrosis score or poor-controlled diabetes had higher risk of elevated baPWV or albuminuria. In conclusion, MAFLD was associated with new-onset elevated baPWV and albuminuria independently of body mass index, waist circumference, and hip circumference. Individuals without NAFLD but diagnosed as MAFLD had high risk of albuminuria, supporting that MAFLD criteria would be practical for the evaluation of long-term risk of subclinical atherosclerosis among fatty liver patients.
|
| Keywords
metabolic dysfunction-associated fatty liver disease
non-alcoholic fatty liver disease
fibrosis score
brachial-ankle pulse wave velocity
albuminuria
|
|
Corresponding Author(s):
Mian Li,Yufang Bi,Zhiyun Zhao
|
|
Just Accepted Date: 18 March 2022
Online First Date: 09 May 2022
Issue Date: 18 November 2022
|
|
| 1 |
M Eslam, AJ Sanyal, J; International Consensus Panel George. MAFLD: a consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology 2020; 158( 7): 1999– 2014.e1
https://doi.org/10.1053/j.gastro.2019.11.312
|
| 2 |
M Eslam, SK Sarin, VW Wong, JG Fan, T Kawaguchi, SH Ahn, MH Zheng, G Shiha, Y Yilmaz, R Gani, S Alam, YY Dan, JH Kao, S Hamid, IH Cua, WK Chan, D Payawal, SS Tan, T Tanwandee, LA Adams, M Kumar, M Omata, J George. The Asian Pacific Association for the Study of the Liver clinical practice guidelines for the diagnosis and management of metabolic associated fatty liver disease. Hepatol Int 2020; 14( 6): 889– 919
https://doi.org/10.1007/s12072-020-10094-2
|
| 3 |
N Mendez-Sanchez, M Arrese, A Gadano, CP Oliveira, E Fassio, JP Arab, NC Chávez-Tapia, M Dirchwolf, A Torre, E Ridruejo, H Pinchemel-Cotrim, Fernández MI Castellanos, M Uribe, M Girala, J Diaz-Ferrer, JC Restrepo, M Padilla-Machaca, L Dagher, M Gatica, B Olaechea, MG Pessôa, M Silva. The Latin American Association for the Study of the Liver (ALEH) position statement on the redefinition of fatty liver disease. Lancet Gastroenterol Hepatol 2021; 6( 1): 65– 72
https://doi.org/10.1016/S2468-1253(20)30340-X
|
| 4 |
G Shiha, K Alswat, Khatry M Al, AI Sharara, N Örmeci, I Waked, M Benazzouz, F Al-Ali, AE Hamed, W Hamoudi, D Attia, M Derbala, M Sharaf-Eldin, SA Al-Busafi, S Zaky, K Bamakhrama, N Ibrahim, Y Ajlouni, M Sabbah, M Salama, A Anushiravani, N Afredj, S Barakat, A Hashim, Y Fouad, R Soliman. Nomenclature and definition of metabolic-associated fatty liver disease: a consensus from the Middle East and north Africa. Lancet Gastroenterol Hepatol 2021; 6( 1): 57– 64
https://doi.org/10.1016/S2468-1253(20)30213-2
|
| 5 |
CW Spearman, H Desalegn, P Ocama, YA Awuku, O Ojo, M Elsahhar, AA Abdo, DA Ndububa, Y Fouad, MM Borodo, M Ng’wanasayi, R Ally, R Elwakil. The sub-Saharan Africa position statement on the redefinition of fatty liver disease: from NAFLD to MAFLD. J Hepatol 2021; 74( 5): 1256– 1258
https://doi.org/10.1016/j.jhep.2021.01.015
|
| 6 |
Y Fouad, R Elwakil, M Elsahhar, E Said, S Bazeed, A Ali Gomaa, A Hashim, E Kamal, M Mehrez, D Attia. The NAFLD-MAFLD debate: eminence vs evidence. Liver Int 2021; 41( 2): 255– 260
https://doi.org/10.1111/liv.14739
|
| 7 |
Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO) European. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J Hepatol 2016; 64( 6): 1388– 1402
https://doi.org/10.1016/j.jhep.2015.11.004
|
| 8 |
M Eslam, PN Newsome, SK Sarin, QM Anstee, G Targher, M Romero-Gomez, S Zelber-Sagi, Wong V Wai-Sun, JF Dufour, JM Schattenberg, T Kawaguchi, M Arrese, L Valenti, G Shiha, C Tiribelli, H Yki-Järvinen, JG Fan, H Grønbæk, Y Yilmaz, H Cortez-Pinto, CP Oliveira, P Bedossa, LA Adams, MH Zheng, Y Fouad, WK Chan, N Mendez-Sanchez, SH Ahn, L Castera, E Bugianesi, V Ratziu, J George. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol 2020; 73( 1): 202– 209
https://doi.org/10.1016/j.jhep.2020.03.039
|
| 9 |
ME Rinella. Nonalcoholic fatty liver disease: a systematic review. JAMA 2015; 313( 22): 2263– 2273
https://doi.org/10.1001/jama.2015.5370
|
| 10 |
G Targher, CD Byrne, A Lonardo, G Zoppini, C Barbui. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: a meta-analysis. J Hepatol 2016; 65( 3): 589– 600
https://doi.org/10.1016/j.jhep.2016.05.013
|
| 11 |
T Ohkuma, T Ninomiya, H Tomiyama, K Kario, S Hoshide, Y Kita, T Inoguchi, Y Maeda, K Kohara, Y Tabara, M Nakamura, T Ohkubo, H Watada, M Munakata, M Ohishi, N Ito, M Nakamura, T Shoji, C Vlachopoulos, A Yamashina, M Nagano, O Yukiyo, T Kabutoya, K Asayama, N Takashima, TT Chowdhury, K Mitsuki-Shinohara, T; Collaborative Group for J-BAVEL (Japan Brachial-Ankle Pulse Wave Velocity Individual Participant Data Meta-Analysis of Prospective Studies) Yamashita. Brachial-ankle pulse wave velocity and the risk prediction of cardiovascular disease: an individual participant data meta-analysis. Hypertension 2017; 69( 6): 1045– 1052
https://doi.org/10.1161/HYPERTENSIONAHA.117.09097
|
| 12 |
K Matsushita, J Coresh, Y Sang, J Chalmers, C Fox, E Guallar, T Jafar, SK Jassal, GW Landman, P Muntner, P Roderick, T Sairenchi, B Schöttker, A Shankar, M Shlipak, M Tonelli, J Townend, Zuilen A van, K Yamagishi, K Yamashita, R Gansevoort, M Sarnak, DG Warnock, M Woodward, J; CKD Prognosis Consortium Ärnlöv. Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: a collaborative meta-analysis of individual participant data. Lancet Diabetes Endocrinol 2015; 3( 7): 514– 525
https://doi.org/10.1016/S2213-8587(15)00040-6
|
| 13 |
J Zheng, Y Zhou, K Zhang, Y Qi, S An, S Wang, X Zhao, YD Tang. Association between nonalcoholic fatty liver disease and subclinical atherosclerosis: a cross-sectional study on population over 40 years old. BMC Cardiovasc Disord 2018; 18( 1): 147
https://doi.org/10.1186/s12872-018-0877-2
|
| 14 |
WH Zhu, LZ Fang, CR Lu, HL Dai, JH Chen, QH Qiao, LY Chen. Correlation between non-alcoholic fatty liver with metabolic risk factors and brachial-ankle pulse wave velocity. World J Gastroenterol 2015; 21( 35): 10192– 10199
https://doi.org/10.3748/wjg.v21.i35.10192
|
| 15 |
N Li, GW Zhang, JR Zhang, D Jin, Y Li, T Liu, RT Wang. Non-alcoholic fatty liver disease is associated with progression of arterial stiffness. Nutr Metab Cardiovasc Dis 2015; 25( 2): 218– 223
https://doi.org/10.1016/j.numecd.2014.10.002
|
| 16 |
SH Kang, KH Cho, JY Do. Non-alcoholic fatty liver disease is associated with low-grade albuminuria in men without diabetes mellitus. Int J Med Sci 2019; 16( 2): 285– 291
https://doi.org/10.7150/ijms.28264
|
| 17 |
M Li, Y Xu, M Xu, L Ma, T Wang, Y Liu, M Dai, Y Chen, J Lu, J Liu, Y Bi, G Ning. Association between nonalcoholic fatty liver disease (NAFLD) and osteoporotic fracture in middle-aged and elderly Chinese. J Clin Endocrinol Metab 2012; 97( 6): 2033– 2038
https://doi.org/10.1210/jc.2011-3010
|
| 18 |
Z Xin, Y Zhu, S Wang, S Liu, M Xu, T Wang, J Lu, Y Chen, Z Zhao, W Wang, G Ning, Y Bi, Y Xu, M Li. Associations of subclinical atherosclerosis with nonalcoholic fatty liver disease and fibrosis assessed by non-invasive score. Liver Int 2020; 40( 4): 806– 814
https://doi.org/10.1111/liv.14322
|
| 19 |
J Ampuero, R Pais, R Aller, R Gallego-Durán, J Crespo, C García-Monzón, J Boursier, E Vilar, S Petta, MH Zheng, D Escudero, JL Calleja, P Aspichueta, M Diago, JM Rosales, J Caballería, J Gómez-Camarero, Iacono O Lo, S Benlloch, A Albillos, J Turnes, JM Banales, V Ratziu, M; HEPAmet Registry Romero-Gómez. Development and validation of hepamet fibrosis scoring system—a simple, noninvasive test to identify patients with nonalcoholic fatty liver disease with advanced fibrosis. Clin Gastroenterol Hepatol 2020; 18( 1): 216– 225.e5
https://doi.org/10.1016/j.cgh.2019.05.051
|
| 20 |
N Stefan. Causes, consequences, and treatment of metabolically unhealthy fat distribution. Lancet Diabetes Endocrinol 2020; 8( 7): 616– 627
https://doi.org/10.1016/S2213-8587(20)30110-8
|
| 21 |
NH Kim, J Park, SH Kim, YH Kim, DH Kim, GY Cho, I Baik, HE Lim, EJ Kim, JO Na, JB Lee, SK Lee, C Shin. Non-alcoholic fatty liver disease, metabolic syndrome and subclinical cardiovascular changes in the general population. Heart 2014; 100( 12): 938– 943
https://doi.org/10.1136/heartjnl-2013-305099
|
| 22 |
HC Hong, SY Hwang, JY Ryu, HJ Yoo, JA Seo, SG Kim, NH Kim, SH Baik, DS Choi, KM Choi. The synergistic impact of nonalcoholic fatty liver disease and metabolic syndrome on subclinical atherosclerosis. Clin Endocrinol (Oxf) 2016; 84( 2): 203– 209
https://doi.org/10.1111/cen.12940
|
| 23 |
K Wijarnpreecha, C Thongprayoon, B Boonpheng, P Panjawatanan, K Sharma, P Ungprasert, S Pungpapong, W Cheungpasitporn. Nonalcoholic fatty liver disease and albuminuria: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol 2018; 30( 9): 986– 994
https://doi.org/10.1097/MEG.0000000000001169
|
| 24 |
Z Liu C Suo O Shi C Lin R Zhao H Yuan L Jin T Zhang X Chen. The health impact of MAFLD, a novel disease cluster of NAFLD, is amplified by the integrated effect of fatty liver disease-related genetic variants. Clin Gastroenterol Hepatol 2020: S1542- 3565(20)31729-8
|
| 25 |
S Lin, J Huang, M Wang, R Kumar, Y Liu, S Liu, Y Wu, X Wang, Y Zhu. Comparison of MAFLD and NAFLD diagnostic criteria in real world. Liver Int 2020; 40( 9): 2082– 2089
https://doi.org/10.1111/liv.14548
|
| 26 |
H Lee, YH Lee, SU Kim, HC Kim. Metabolic dysfunction-associated fatty liver disease and incident cardiovascular disease risk: a nationwide cohort study. Clin Gastroenterol Hepatol 2020; S1542-3565( 20): 31717– 1
|
| 27 |
N Stefan, HU Häring, K Cusi. Non-alcoholic fatty liver disease: causes, diagnosis, cardiometabolic consequences, and treatment strategies. Lancet Diabetes Endocrinol 2019; 7( 4): 313– 324
https://doi.org/10.1016/S2213-8587(18)30154-2
|
| 28 |
Y Chen, M Xu, T Wang, J Sun, W Sun, B Xu, X Huang, Y Xu, J Lu, X Li, W Wang, Y Bi, G Ning. Advanced fibrosis associates with atherosclerosis in subjects with nonalcoholic fatty liver disease. Atherosclerosis 2015; 241( 1): 145– 150
https://doi.org/10.1016/j.atherosclerosis.2015.05.002
|
| 29 |
S Yamamura, M Eslam, T Kawaguchi, T Tsutsumi, D Nakano, S Yoshinaga, H Takahashi, K Anzai, J George, T Torimura. MAFLD identifies patients with significant hepatic fibrosis better than NAFLD. Liver Int 2020; 40( 12): 3018– 3030
https://doi.org/10.1111/liv.14675
|
|
Viewed |
|
|
|
Full text
|
|
|
|
|
Abstract
|
|
|
|
|
Cited |
|
|
|
|
| |
Shared |
|
|
|
|
| |
Discussed |
|
|
|
|