|
|
|
Hemophagocytic lymphohistiocytosis: critical reappraisal of a potentially under-recognized condition |
Somanath Padhi1( ), Renu G’ Boy Varghese1, Anita Ramdas1, Manjiri Dilip Phansalkar1, RajLaxmi Sarangi2 ), Renu G’ Boy Varghese1, Anita Ramdas1, Manjiri Dilip Phansalkar1, RajLaxmi Sarangi2 |
| 1. Department of Pathology, Pondicherry Institute of Medical Sciences, Ganapathichettykulam, Kalapet, Puducherry 605 014, India; 2. Department of Biochemistry, Pondicherry Institute of Medical Sciences, Ganapathichettykulam, Kalapet, Puducherry 605 014, India |
|
|
|
|
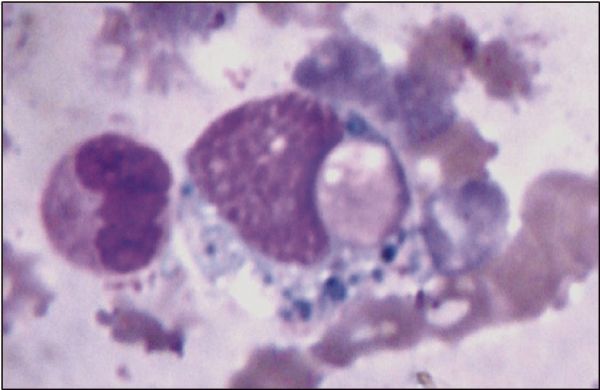
Abstract Hemophagocytic lymphohistiocytosis (HLH) is an uncommon, potentially life threatening, hyper inflammatory syndrome of diverse etiologies. Cardinal signs include prolonged fever, organomegaly, and persistent unexplained cytopenias. In spite of the well known diagnostic criteria put forth by HLH society, this continues to pose great diagnostic challenge in both pediatric and adult intensive care settings. We describe 4 adult (2 males, 2 females, aged 19, 29, 40, and 17 years) and 3 pediatric (2 males, 1female, aged 1 month, 6 months, and 12 years) patients with secondary HLH who satisfied the HLH-2004 diagnostic criteria. Definite evidence of hemophagocytosis was noted in 4 patients on initial bone marrow examination. The underlying etiologies were as follows: Rickettsia tsutsugamushi (case 1), autoimmune disorder (case 2), systemic onset juvenile idiopathic arthritis (sJIA) (case 3), unknown bite (possibly a venomous snake) (case 4), Plasmodium vivax (case 5), Cytomegalo virus (case 6), and Mycobacterium tuberculosis (case 7). In one patient, hemophagocytosis was presumed to have been exacerbated by administration of granulocyte monocyte colony stimulating factor (GM-CSF) for severe neutropenia. Two patients died with disseminated intravascular coagulation (DIC) and multi organ failure within few days of HLH diagnosis. Immunosuppressive therapy was started in 3 patients, and etoposide was started in one patient only. Due to lack of specificity of diagnostic criteria, diagnosing and differentiating HLH from its closest mimickers like sepsis/septic shock may be quite challenging in critically ill patients. Therefore, increasing awareness among physicians is essential for early diagnosis and effective therapy to reduce the mortality.
|
| Keywords
hemophagocytic lymphohistiocytosis
diagnosis
therapy
GM-CSF
bone marrow
|
|
Corresponding Author(s):
Padhi Somanath,Email:somanath.padhi@gmail.com
|
|
Issue Date: 05 December 2013
|
|
| 1 |
Janka G. Hemophagocytic lymphohistiocytosis: when the immune system runs amok. Klin Padiatr 2009; 221(5): 278–285
doi: 10.1055/s-0029-1237386 pmid:19707989
|
| 2 |
Machaczka M. Genetic and acquired hemophagocytic lymphohistiocytosis. Int Rev Allergol Clin Immunol 2011; 17(3–4): 63–69
|
| 3 |
Tseng YT, Sheng WH, Lin BH, Lin CW, Wang JT, Chen YC, Chang SC. Causes, clinical symptoms, and outcomes of infectious diseases associated with hemophagocytic lymphohistiocytosis in Taiwanese adults. J Microbiol Immunol Infect 2011; 44(3): 191–197
doi: 10.1016/j.jmii.2011.01.027 pmid:21524613
|
| 4 |
Glasser L, Legolvan M, Horwitz HM. Florid histiocytic hemophagocytosis following therapy with long acting G-CSF (pegfilgrastim). Am J Hematol 2007; 82(8): 753–757
doi: 10.1002/ajh.20854 pmid:17315211
|
| 5 |
Wang S, Degar BA, Zieske A, Shafi NQ, Rose MG. Hemophagocytosis exacerbated by G-CSF/GM-CSF treatment in a patient with myelodysplasia. Am J Hematol 2004; 77(4): 391–396
doi: 10.1002/ajh.20202 pmid:15551287
|
| 6 |
Henter JI, Horne A, Aricó M, Egeler RM, Filipovich AH, Imashuku S, Ladisch S, McClain K, Webb D, Winiarski J, Janka G. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer 2007; 48(2): 124–131
doi: 10.1002/pbc.21039 pmid:16937360
|
| 7 |
Filipovich AH. Hemophagocytic lymphohistiocytosis (HLH) and related disorders. Hematology (Am Soc Hematol Educ Program) 2009; 2009(1): 127–131
doi: 10.1182/asheducation-2009.1.127 pmid:20008190
|
| 8 |
Créput C, Galicier L, Buyse S, Azoulay E. Understanding organ dysfunction in hemophagocytic lymphohistiocytosis. Intensive Care Med 2008; 34(7): 1177–1187
doi: 10.1007/s00134-008-1111-y pmid:18427781
|
| 9 |
Raschke RA, Garcia-Orr R. Hemophagocytic lymphohistiocytosis: a potentially underrecognized association with systemic inflammatory response syndrome, severe sepsis, and septic shock in adults. Chest 2011; 140(4): 933–938
doi: 10.1378/chest.11-0619 pmid:21737492
|
| 10 |
Gurion R, Lehman TJ, Moorthy LN. Systemic arthritis in children: a review of clinical presentation and treatment. Int J Inflam 2012; 2012:271569
|
| 11 |
Gupta S, Weitzman S. Primary and secondary hemophagocytic lymphohistiocytosis: clinical features, pathogenesis and therapy. Expert Rev Clin Immunol 2010; 6(1): 137–154
doi: 10.1586/eci.09.58 pmid:20383897
|
| 12 |
Buyse S, Teixeira L, Galicier L, Mariotte E, Lemiale V, Seguin A, Bertheau P, Canet E, de Labarthe A, Darmon M, Rybojad M, Schlemmer B, Azoulay E. Critical care management of patients with hemophagocytic lymphohistiocytosis. Intensive Care Med 2010; 36(10): 1695–1702
doi: 10.1007/s00134-010-1936-z pmid:20532477
|
| 13 |
Kuwata K, Yamada S, Kinuwaki E, Naito M, Mitsuya H. Peripheral hemophagocytosis: An early indicator of advanced systemic inflammatory response syndrome/hemophagocytic syndrome. Shock 2006; 25(4): 344–350
doi: 10.1097/01.shk.0000209520.82377.41 pmid:16670635
|
| 14 |
To KK, Hung IF, Li IW, Lee KL, Koo CK, Yan WW, Liu R, Ho KY, Chu KH, Watt CL, Luk WK, Lai KY, Chow FL, Mok T, Buckley T, Chan JF, Wong SS, Zheng B, Chen H, Lau CC, Tse H, Cheng VC, Chan KH, Yuen KY. Delayed clearance of viral load and marked cytokine activation in severe cases of pandemic H1N1 2009 influenza virus infection. Clin Infect Dis 2010; 50(6): 850–859
doi: 10.1086/650581 pmid:20136415
|
| 15 |
Takahashi N, Chubachi A, Kume M, Hatano Y, Komatsuda A, Kawabata Y, Yanagiya N, Ichikawa Y, Miura AB, Miura I. A clinical analysis of 52 adult patients with hemophagocytic syndrome: the prognostic significance of the underlying diseases. Int J Hematol 2001; 74(2): 209–213
doi: 10.1007/BF02982007 pmid:11594524
|
| 16 |
Dhote R, Simon J, Papo T, Detournay B, Sailler L, Andre MH, Dupond JL, Larroche C, Piette AM, Mechenstock D, Ziza JM, Arlaud J, Labussiere AS, Desvaux A, Baty V, Blanche P, Schaeffer A, Piette JC, Guillevin L, Boissonnas A, Christoforov B. Reactive hemophagocytic syndrome in adult systemic disease: report of twenty-six cases and literature review. Arthritis Rheum 2003; 49(5): 633–639
doi: 10.1002/art.11368 pmid:14558048
|
| 17 |
Kaito K, Kobayashi M, Katayama T, Otsubo H, Ogasawara Y, Sekita T, Saeki A, Sakamoto M, Nishiwaki K, Masuoka H, Shimada T, Yoshida M, Hosoya T. Prognostic factors of hemophagocytic syndrome in adults: analysis of 34 cases. Eur J Haematol 1997; 59(4): 247–253
doi: 10.1111/j.1600-0609.1997.tb00984.x pmid:9338623
|
| 18 |
Shea YF, Chan JFW, Kwok WC, Hwang YY, Chan TC, Ni MYX, Li IWS, Chiu PKC, Luk JKH, Chu LW. Haemophagocytic lymphohistiocytosis: an uncommon clinical presentation of tuberculosis. Hong Kong Med J 2012; 18(6): 517–525
pmid:23223654
|
| 19 |
Castillo L, Carcillo J. Secondary hemophagocytic lymphohistiocytosis and severe sepsis/ systemic inflammatory response syndrome/multiorgan dysfunction syndrome/macrophage activation syndrome share common intermediate phenotypes on a spectrum of inflammation. Pediatr Crit Care Med 2009; 10(3): 387–392
doi: 10.1097/PCC.0b013e3181a1ae08 pmid:19325510
|
| 20 |
Castillo L. High elevated ferritin levels and the diagnosis of HLH/Sepsis/SIRS/MODS/MAS. Pediatr Blood Cancer 2008; 51(5): 710–711, author reply 710–711
doi: 10.1002/pbc.21681 pmid:18615508
|
| 21 |
Allen CE, Yu X, Kozinetz CA, McClain KL. Highly elevated ferritin levels and the diagnosis of hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer 2008; 50(6): 1227–1235
doi: 10.1002/pbc.21423 pmid:18085676
|
| 22 |
Hahn YS, Kim JG. Pathogenesis and clinical manifestations of juvenile rheumatoid arthritis. Korean J Pediatr 2010; 53(11): 921–930
doi: 10.3345/kjp.2010.53.11.921 pmid:21218013
|
|
Viewed |
|
|
|
Full text
|
|
|
|
|
Abstract
|
|
|
|
|
Cited |
|
|
|
|
| |
Shared |
|
|
|
|
| |
Discussed |
|
|
|
|